At its core, the Stark Law is a federal regulation designed to eliminate conflicts of interest from physician referrals. Specifically, it prohibits a physician from referring Medicare or Medicaid patients for designated health services to an entity with which the physician—or an immediate family member—has a financial relationship.
It’s a strict liability statute, a critical distinction for executives. Unlike other fraud and abuse laws, intent is irrelevant. If the elements of a prohibited referral are present and no exception applies, a violation has occurred, regardless of intent.
Decoding The Stark Law for Healthcare Leaders
For any healthcare executive or clinical leader, the Stark Law isn't just another line item in the compliance manual. It's a fundamental business constraint that shapes how organizations structure everything from physician employment contracts to joint ventures and service line development.
Its primary purpose is to remove financial incentives from medical decision-making. The goal is to ensure clinical services are ordered based on medical necessity, not because they generate revenue for the referring physician. This principle protects the financial integrity of federal healthcare programs.
To fully appreciate its impact, one must look at its history. Congress passed the Ethics in Patient Referrals Act in 1989 after studies showed self-referring physicians were ordering up to 45% more lab tests than their non-conflicted peers, driving up Medicare expenditures. This initial version, often called Stark I, took direct aim at clinical laboratory services to curb this overutilization.
Foundational Concepts for Executives
The entire statute is built on three core components. If all three of these exist—and the arrangement does not fit squarely within a specific exception—a violation has occurred.
- A Physician Referral: This is a request or order from a physician for an item or service that is payable by Medicare or Medicaid.
- A Financial Relationship: This is broadly defined and includes direct ownership or investment interests, as well as any compensation arrangement between the physician (or their immediate family) and the entity.
- Designated Health Services (DHS): This is a specific list of 10 categories of services, including clinical labs, physical therapy, radiology, durable medical equipment (DME), and both inpatient and outpatient hospital services. If the referral is not for a DHS, Stark Law is not implicated.
The Stark Law operates on a "strict liability" basis. Unlike other fraud and abuse laws, the government does not need to prove corrupt intent. If the referral, financial relationship, and DHS elements exist without a valid exception, a violation has occurred.
Given the density of these regulations, healthcare leaders must master the art of reading and summarizing dense texts to quickly extract key business implications. The table below offers a high-level reference for these core concepts.
Stark Law Core Components At A Glance
This table breaks down the foundational elements of the Stark Law, providing executives a quick reference to its main pillars.
| Component | Description for Healthcare Executives |
|---|---|
| Physician Referral | Any request by a physician for a Medicare/Medicaid-payable item or service. This is the initial action that triggers Stark Law scrutiny. |
| Financial Relationship | Includes any direct/indirect ownership, investment, or compensation arrangement between the physician (or an immediate family member) and the entity providing the service. It’s a very broad definition. |
| Designated Health Services (DHS) | A specific list of 10 services, including labs, imaging, PT/OT, DME, and hospital services. If the service isn't on this list, the Stark Law doesn't apply to the referral. |
| Strict Liability | The "no-fault" nature of the law. A violation doesn't require bad intent. If the technical elements are met and no exception applies, a violation has occurred, period. |
Grasping these concepts is the first step toward building a compliant organization. This isn't just about avoiding massive penalties; it's about building an ethical, patient-first business that can withstand regulatory scrutiny.
The Anatomy of a Stark Law Violation
To manage risk effectively, executives must first understand its components. A Stark Law violation is not a single misstep but the convergence of three specific elements. Think of it as a three-legged stool: if all three legs are present without the support of a legal exception, the arrangement is non-compliant and will collapse under regulatory pressure.
This framework provides a clear, repeatable process for internal audits. Every physician arrangement and referral pattern must be examined through this three-part lens to identify weaknesses before they become costly liabilities.
The First Element: A Physician Referral
It all begins with a physician referral. The law defines this broadly as any request, order, or certification from a physician for an item or service payable by Medicare or Medicaid. This includes not just explicit orders but also the establishment of a plan of care that "includes" the provision of a DHS.
The term "physician" is also specific, covering medical doctors, osteopaths, dentists, podiatrists, optometrists, and chiropractors. Any referral from one of these professionals for a federally covered service constitutes the first piece of the puzzle.
The Second Element: Designated Health Services
Next, the referral must be for a Designated Health Service (DHS). If the service is not on this specific government list, the Stark Law does not apply. The list was curated to target services historically prone to overutilization when financial incentives were present.
The scope of DHS expanded significantly with the update known as Stark II. This expansion, passed in the Omnibus Budget Reconciliation Act of 1993, stretched the law beyond its initial focus on clinical labs. It grew to cover a much wider range of services—such as radiology, therapy, and hospital care—while also applying the rules to Medicaid patients.
This was a direct legislative response to escalating federal healthcare costs, particularly after data showed that self-referrals were linked to 30-50% higher service volumes in areas like diagnostic imaging.
The key DHS categories to monitor are:
- Clinical laboratory services
- Physical therapy, occupational therapy, and speech-language pathology services
- Radiology and certain other imaging services (including MRI and CT scans)
- Radiation therapy services and supplies
- Durable medical equipment (DME) and supplies
- Parenteral and enteral nutrients, equipment, and supplies
- Prosthetics, orthotics, and prosthetic devices and supplies
- Home health services
- Outpatient prescription drugs
- Inpatient and outpatient hospital services
This diagram illustrates how the three core components—the referral, the financial link, and the DHS—must all connect for a violation to occur.
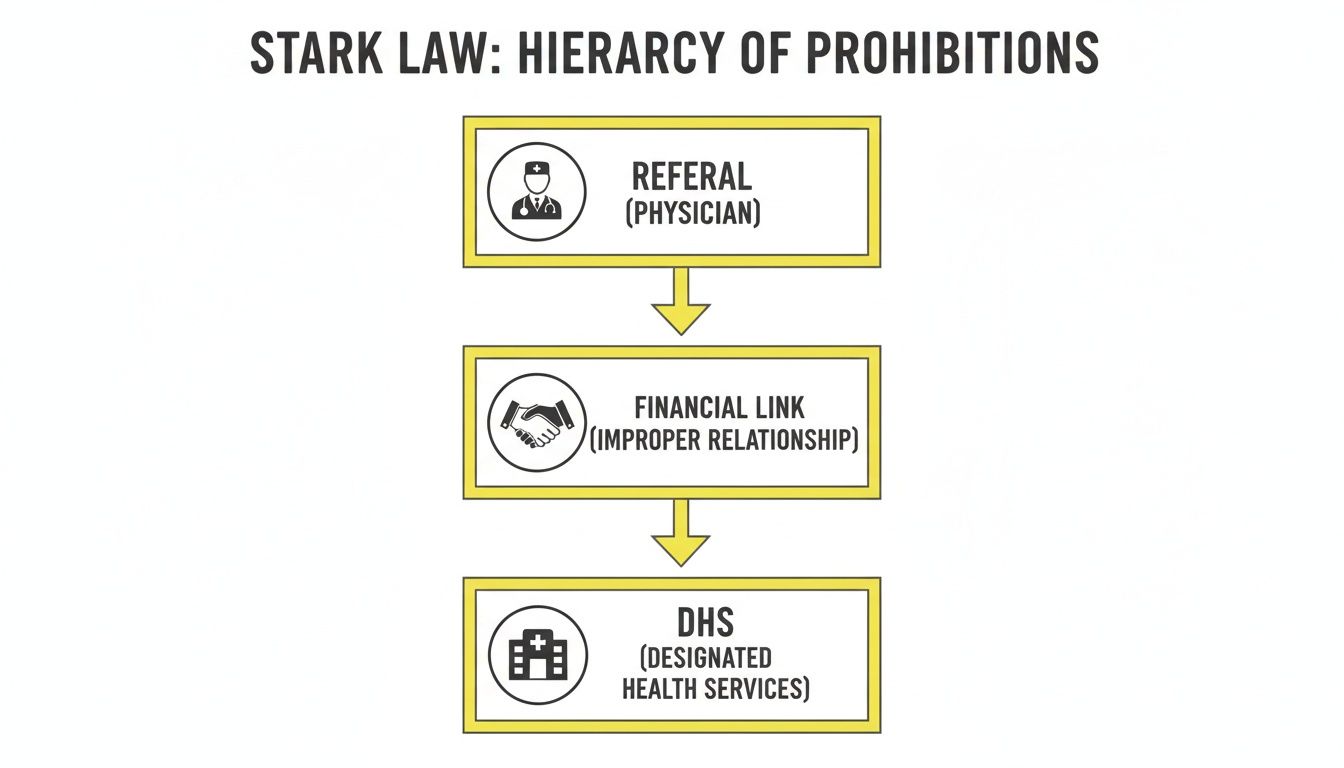
This serves as an effective visual checklist. A violation only exists when all three elements are simultaneously present.
The Third Element: A Financial Relationship
The final and most complex element is a financial relationship between the referring physician (or their immediate family) and the entity providing the DHS. This is where most organizations inadvertently fall into non-compliance.
A "financial relationship" is not limited to physician ownership in a facility. The definition is incredibly broad, capturing nearly any financial interaction imaginable.
A "financial relationship" can be a direct ownership or investment interest in the entity, but it also includes any compensation arrangement. This means salaries, bonuses, directorship fees, consulting agreements, or even below-market-rate office leases can trigger the law.
These relationships can be direct or indirect, adding another layer of complexity. An indirect relationship might exist if compensation flows through intermediary entities but remains tied to the volume or value of referrals the physician generates. This expansive definition necessitates a meticulous review of every financial tie to ensure compliance.
Finding Safe Harbor With Stark Law Exceptions

Navigating the Stark Law is not about halting physician collaborations; it's about structuring them correctly. The statute includes numerous exceptions that function as “safe harbors,” creating protected pathways for legitimate and necessary business arrangements.
Think of these exceptions as pre-approved blueprints for compliance. If a financial arrangement meets every technical requirement of a specific exception, it is legally shielded from Stark’s prohibitions—even if it involves a physician referring for designated health services (DHS). For healthcare leaders, mastering these exceptions is the key to building integrated care models without incurring regulatory risk.
These are not loopholes. They were intentionally designed to protect common and beneficial healthcare arrangements from being unduly restricted.
The Bona Fide Employment Exception
One of the most frequently used safe harbors is the bona fide employment exception. This allows a hospital or group practice to employ a physician and compensate them for their services, even if that physician refers patients for DHS back to the employing organization.
However, this is not a blanket approval. The arrangement must meet several strict criteria:
- Identifiable Services: The employment must be for specific, identifiable services.
- Commercially Reasonable: The compensation must be commercially reasonable, even if the physician generated zero referrals.
- Fair Market Value: The compensation must be consistent with fair market value (FMV) and, critically, must not be determined in a manner that takes into account the volume or value of referrals.
In practical terms, a physician cannot be paid a commission on the downstream revenue from the MRIs or lab tests they order. While compensation can be tied to a physician's personal productivity, it cannot be linked to the revenue from their DHS referrals.
Personal Service and Fair Market Value Exceptions
For arrangements with independent contractors, such as medical directorships or specialized consulting agreements, the personal service arrangements exception and the fair market value compensation exception are crucial. These often work in tandem.
To qualify, the arrangement must satisfy several core requirements:
- Written Agreement: The arrangement must be detailed in a signed, written contract that specifies all services to be provided.
- Term of Agreement: The contract must have a term of at least one year.
- Aggregate Compensation: The total compensation must be set in advance, be consistent with fair market value, and not be determined by the volume or value of referrals.
The concept of Fair Market Value is the absolute cornerstone of most Stark Law exceptions. It’s defined as the price a service would command in an arm's-length transaction on the open market. Obtaining an independent, third-party FMV opinion for physician arrangements is a critical step in building a defensible compliance strategy.
Navigating Value-Based Care Arrangements
As the industry pivots from fee-for-service to value-based care, regulators recognized that the existing rules were misaligned with new delivery models. Recent updates to the Stark Law created new, permanent exceptions specifically designed to support value-based enterprises (VBEs). These safe harbors permit financial arrangements that directly promote care coordination and improved patient outcomes.
To see how these models work in practice, it’s worth exploring an inside look at a value-based playbook. The new exceptions are tiered based on the level of financial risk the VBE assumes, granting greater flexibility to organizations that take on full financial responsibility for patient populations.
These modern rules acknowledge that in a value-based system, financial integration is necessary to align incentives and improve care delivery. For executives leading modern healthcare organizations, understanding these safe harbors is fundamental.
Stark Law Versus The Anti-Kickback Statute
It is easy to conflate the Stark Law with the Anti-Kickback Statute (AKS). Both laws target improper financial arrangements in healthcare, but confusing them is a common—and potentially catastrophic—mistake for any healthcare leader.
They operate on fundamentally different legal principles. Grasping the distinction is the first step toward building a robust and effective compliance program.
An Analogy: Traffic Laws vs. Bribery Laws
The simplest way to differentiate them is through an analogy.
Think of the Stark Law as a strict traffic law. If you drive through a red light, you receive a citation. It does not matter if you were distracted, in a hurry, or simply failed to see it. Your intent is irrelevant; the act itself constitutes the violation. You violated the rule and must pay the penalty.
The Anti-Kickback Statute, in contrast, is analogous to a bribery law. To secure a conviction, a prosecutor must prove corrupt intent. They must demonstrate that an individual knowingly and willfully offered or accepted something of value to induce referrals. Here, intent is the central element.
Key Differences in Scope and Intent
The Stark Law is a civil statute with a narrow focus. It applies only to referrals from physicians for a specific list of Designated Health Services (DHS) when those services are paid by Medicare or Medicaid. Because it’s a strict liability law, if the technical elements of an improper referral are met, a violation has occurred.
The AKS is a criminal statute with a much broader reach. It applies to anyone who influences referrals for any item or service covered by a federal healthcare program. This includes not just physicians but also hospital executives, lab owners, device representatives, and marketing consultants.
The core distinction comes down to intent and scope. Stark is a civil, no-fault law focused on physician self-referrals for DHS. The AKS is a criminal law that requires proof of corrupt intent and covers all federal healthcare business generated by anyone.
Penalties and Enforcement Actions
Because one is a civil law and the other is criminal, their penalties differ significantly.
A Stark Law violation typically results in financial penalties. This includes repayment of all claims stemming from improper referrals, plus substantial fines for each claim submitted. These penalties can easily run into the millions of dollars but do not involve incarceration.
An AKS violation is an entirely different matter. As a criminal offense, it carries far more severe consequences: massive fines, exclusion from federal healthcare programs, and—most critically—prison sentences. A single violation can threaten an organization's existence and an executive's personal freedom.
The table below summarizes these differences for a side-by-side comparison.
Stark Law vs Anti-Kickback Statute: A Comparison for Leaders
This direct comparison highlights the fundamental differences between the Stark Law and the Anti-Kickback Statute for quick executive reference.
| Attribute | Stark Law | Anti-Kickback Statute (AKS) |
|---|---|---|
| Nature of Law | Civil Statute | Criminal Statute |
| Intent Requirement | Strict Liability (No intent required) | Specific Intent (Must prove "knowing and willful" misconduct) |
| Scope of Application | Only applies to physician referrals for DHS | Applies to anyone who influences referrals for any federally payable item/service |
| Primary Penalties | Fines, repayment of claims, exclusion | Fines, imprisonment, exclusion |
It is crucial to remember that a single financial arrangement can violate both laws simultaneously. An effective compliance strategy must analyze every physician relationship through two distinct lenses: the strict, technical framework of the Stark Law and the intent-based analysis of the AKS. Anything less leaves the organization dangerously exposed.
The High Cost of Non-Compliance
Nothing motivates a commitment to compliance quite like understanding the consequences of a Stark Law violation. These are not abstract warnings or minor fines. The penalties are severe, multi-layered, and designed to impact a healthcare organization's finances and operational viability.
A violation triggers a devastating cascade of penalties that can easily spiral into the millions, posing a direct threat to an organization's stability and reputation.
The Financial Fallout of a Violation
The initial penalty is the mandatory repayment of all claims tied to the improper referrals. Every dollar paid by Medicare or Medicaid for those non-compliant services must be returned. While this alone can be a crippling amount, it is only the beginning.
On top of repayments, the government imposes civil monetary penalties (CMPs). These fines can be as high as $15,000 for each service billed pursuant to the prohibited arrangement. For an organization with even a moderate referral volume, these per-claim penalties accumulate rapidly.
Furthermore, a penalty of up to $100,000 can be assessed for each arrangement or scheme intentionally designed to circumvent the law. This targets deliberate workarounds, not inadvertent errors.
The False Claims Act Multiplier
This is where the financial risk escalates dramatically. A Stark Law violation often becomes entangled with the False Claims Act (FCA). Because every claim submitted resulting from an improper referral is considered "false or fraudulent," it creates FCA liability. This transforms a difficult situation into a potential catastrophe.
Under the FCA, penalties can surge to three times the amount of the damages sustained by the government, plus thousands more in fines per claim. This “treble damages” provision is what turns a massive repayment obligation into a potentially bankrupting event.
These are not empty threats. Enforcement actions have recovered staggering sums, underscoring the government's focus on fraud in a system where Medicare spending reached $944 billion in 2023. Between 2000 and 2020, the Department of Justice and CMS settled over 100 cases involving Stark Law, recovering more than $2.5 billion. A textbook example is the 2019 case against Tuomey Healthcare, which resulted in a $237 million settlement—all stemming from improper referrals that had generated just $47 million in Medicare revenue. You can find more details about how the government enforces the Stark law in healthcare on medprosystems.com.
Real-World Cautionary Tales
These penalties are very real. Numerous healthcare organizations have learned this the hard way, leaving behind cautionary tales. These cases often demonstrate how seemingly minor oversights—a poorly structured physician contract, a flawed profit-sharing model—can explode into multi-million dollar settlements.
- A Hospital System's Misstep: One major hospital system paid tens of millions to settle allegations that its physician compensation plans were not at fair market value and were instead tied to referral volume for services like imaging and labs.
- A Physician Group's Costly Error: A large specialty practice was hit with a multi-million dollar settlement after its profit-sharing methodology was found to distribute revenue from ancillary services in a way that directly violated Stark's strict rules.
Beyond the financial devastation, a violation inflicts deep and lasting damage to an organization's reputation. It shatters trust with patients, referring physicians, and partners, making it incredibly difficult to recruit top talent or maintain standing in the community long after the financial penalties are paid.
Building Your Stark Law Compliance Playbook
When it comes to the Stark Law, a proactive defense is the only viable strategy. Waiting to react to an audit or investigation is a losing proposition. The objective is to build a robust, forward-thinking compliance program that identifies and neutralizes risks before they materialize into threats.
This is not merely about avoiding penalties; it is about embedding operational integrity into the organization's culture.
Core Pillars of an Effective Strategy
An effective program is built on several non-negotiable pillars. The first is a commitment to regular, rigorous audits of all physician financial arrangements. This requires a deep dive into every contract to ensure it fits squarely within a recognized Stark Law exception.
Next, you need an ironclad process for verifying fair market value (FMV) and commercial reasonableness for all physician compensation. This cannot be an afterthought. Obtaining independent, third-party FMV opinions for physician contracts is a critical defensive measure, creating a defensible position if arrangements are ever questioned.
Finally, meticulous documentation is your greatest asset. Every agreement, payment, and FMV analysis must be documented, filed, and maintained. This paper trail serves as front-line evidence that arrangements were structured in good faith and with compliant intent. These records must be organized and easily retrievable.
A well-documented compliance program transforms your defense from "we believe we were compliant" to "here is the evidence that proves we were compliant." That distinction is everything when regulators come knocking.
For a deeper dive into managing these kinds of risks, check out a practical guide to regulatory compliance risk management.
A Practical Compliance Checklist
How does your organization's framework measure up? Use this checklist to identify potential gaps.
- Centralized Contract Management: Do you have a single, organized system for managing all physician contracts and financial arrangements? Or are they siloed across different departments?
- Mandatory FMV Reviews: Does every physician compensation arrangement undergo a formal fair market value and commercial reasonableness review before execution?
- Regular Audits: Do you conduct periodic internal audits designed to stress-test your arrangements against specific Stark Law exceptions?
- Clear Documentation Policies: Are there clear, enforced policies for documenting the legitimate business need for every physician arrangement?
- Ongoing Education: Do your executives, administrators, and physicians receive regular training on Stark Law fundamentals and internal compliance policies?
These contracts are the foundation of your compliance efforts. For a closer look at structuring them correctly, our guide on collaborating physician contracts offers valuable insights.
Leveraging the Self-Disclosure Protocol
Even with the best program, errors can occur. When a potential violation is discovered, the CMS Voluntary Self-Referral Disclosure Protocol (SRDP) is an essential tool.
The SRDP allows organizations to voluntarily report potential violations, which can lead to significantly reduced settlement amounts. More importantly, utilizing the SRDP demonstrates good faith and a commitment to compliance. It transforms a potential crisis into a manageable, corrective action. It is a strategic tool that must be part of any serious compliance playbook, offering a clear path to resolve issues and limit financial exposure.
Key Stark Law Questions for Executives
As a leader, your focus is on strategy and risk management. Regarding the Stark Law, a few high-level questions consistently arise. Obtaining clear answers is non-negotiable for sound decision-making.
Does Stark Law Apply to Private Payers?
This is a common blind spot. Many executives assume the Stark Law is strictly a Medicare and Medicaid issue. While that is true for the federal statute, this view is dangerously narrow.
The reality is that many states have their own "mini-Stark" laws. These state-level statutes often extend similar—or even stricter—prohibitions to cover all payers, including commercial insurance. This makes a comprehensive, payer-agnostic compliance strategy a business necessity. Ignoring these state laws creates significant financial and legal exposure.
How Does Value-Based Care Change the Game?
The industry’s shift toward value-based care created a direct conflict with the Stark Law's traditional fee-for-service framework. To resolve this, regulators have modernized the rules, creating new safe harbors designed specifically for value-based arrangements.
These changes provide crucial flexibility to build clinically integrated networks and Accountable Care Organizations (ACOs). They permit financial arrangements that promote care coordination and reward positive outcomes, which was previously challenging under the old rules.
The core prohibitions of the law remain, but these new exceptions acknowledge a critical reality: in a value-based model, some financial alignment is essential for improving care and controlling costs. These safe harbors are the bedrock for any organization transitioning away from traditional payment models.
Distinguishing Ownership from Compensation
The Stark Law casts a wide net over financial relationships, separating them into two main categories: ownership/investment and compensation. Both demand equal scrutiny, as either can trigger a violation.
Ownership or Investment Interest: This is relatively straightforward. It includes holding equity, stock, or a partnership share in an entity. Debt instruments like bonds are also included.
Compensation Arrangement: This category is far broader and more complex. It covers any form of remuneration—direct or indirect, overt or covert, in cash or in kind. This means everything from a physician’s salary and bonuses to office lease agreements and medical directorship fees is subject to the law.
Understanding that any flow of value can create a financial relationship is the first step in a thorough compliance audit. Both direct ownership stakes and compensation arrangements must be carefully structured to fit squarely within a specific Stark Law exception. If they do not, the arrangement is non-compliant.
At ClinX Academy, we translate complex healthcare regulations into the practical business fluency you need to lead with confidence. Our accelerated, virtual Mini Healthcare MBA equips you with the actionable knowledge to navigate compliance, operations, and payment models effectively. Learn more and enroll at ClinX Academy.